
December 2021
Greetings International Oral Lichen Planus Support Group! December 2021
As we end another year, we wish to recognize all of you who continue to support us through emails, progress reports and thank you notes. Since the last webinar we provided, many new members have asked to be added to our newsletter. This newsletter not only reaches the United States, but we have many members in other countries who write to us and ask for opinions/referrals.
On this holiday season, we are very sad to announce that my co-founder and co-host, Dr. Terry Rees passed away on November 15th, 2021. A memorial for Dr. Rees occurred on November 19th in Dallas, Texas with his beloved wife, Greta Rees and his children, grandchildren, and great grandchildren in attendance. Dr. Rees was the founder of the stomatology clinic at the dental college in Dallas and was my co-host for the International Oral Lichen Planus Support Group that we founded in 1997. The service was beautiful, and we will greatly miss him. You can read his biography on the site under co-host information. Dr. Rees contributed so much to research, teaching and to the dental community. His death is a tremendous loss.
We provided a webinar in October featuring Dr. Paras Patel that is also posted on the IOLPSG site. Dr. Patel is involved in the treatment of oral lichen planus, but he also has the added benefit of actually reading the tissue samples that come through the biopsy service at Texas A&M College of Dentistry-Department of Oral Pathology since he is an oral pathologist at the college. He treats patients and also participates in the stomatology clinic. Many of you have contacted us and we received so many requests for more of these virtual webinars. Dr. Patel will also act as a regular for our webinars and assist in providing current information about lichen planus as we proceed. The new year will bring more participants and more clinical information on oral lichen planus. Please let us know your thoughts on any issues related to lichen planus and any questions that you may have for us. Dawn Lewis, , of Limitless Grit Corp, served as a moderator for the webcast and we will ask her to join us for future webcasts.
To provide more of these features in the coming years, please consider us in your “end of the year” donations. No contribution is considered too small. We are asking you to make your donation to: The International Oral Lichen Planus Support Group. Your checks can be sent in care of The Department of Periodontics, Attention: Ms. Holly Chiem, 3302 Gaston Ave. Dallas, TX 75246. Holly is the administrative assistant for the department and will deposit these into our account. We appreciate the past donations that you have contributed, and we will use this fund toward improving and sustaining the existing support group. We are using this method rather than the existing buttons on the site that many of you have found confusing or vague with regard to contributions.
We would like to provide more information from other countries regarding what they are recommending for patients. Since we get many emails from those under treatment or seeking treatment/referrals, adding this element helps us in other treatment options/recommendations. The support group is international and we hope to add more of this focus in future webinars and newsletters. Please see the attachment from a doctor in Medellin, Columbia, Dr. Jairo Robledo-Sierra | DDS, MSc (OralMed), PhD www.ces.edu.co
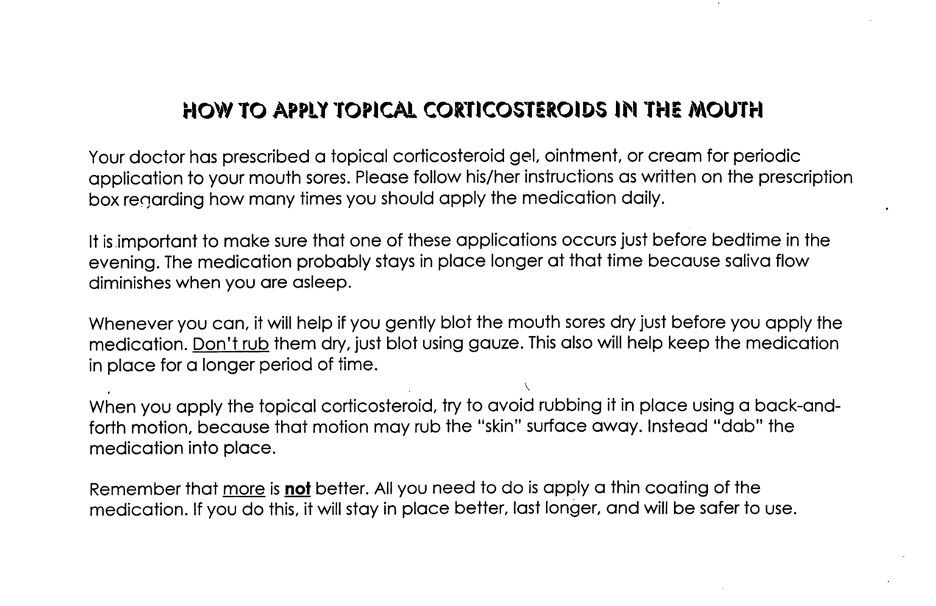
- Included in this newsletter is the correct way to apply corticosteroids orally.
- Maintenance Guidelines
- Reducing Stain on Your Teeth.
- Treatment options in Sweden and Columbia
We wish all of you a wonderful holiday season with family and friends. The holidays can be a stressful time, so please take care of yourself. We are always available to assist you with referrals and advice regarding your oral concerns.
Nancy W. Burkhart
Dr. Nancy W. Burkhart, Ed.D, M.Ed., BS, AFAAOM
Department of Periodontics, Adjunct Professor
College of Dentistry, Texas A&M University
3302 Gaston Ave.
Dallas Texas 75246
nancy.burkhart@tamu.edu
The International Oral Lichen Planus Support Group
https://dentistry.tamu.edu/olp/index.html
Maintenance Appointment Guidelines for the Patient with a Mucosal Disorder
- Patients should have professional cleanings and exams every 2 to 3 months. Periodontal patients may need to be seen every 2 months, depending upon the patient's status and periodontal health.
- The practitioner should note any areas that are in contact with sharp edges, crowns, or restorative materials. This is routinely performed during a dental exam.
- All soft tissue areas should be evaluated. Findings should be described and recorded, with any suspicious areas being reevaluated. Careful evaluation for Candida is suggested, especially for patients who are using topical corticosteroids. Candida infection is often noted and is especially prevalent in long-term steroid use.
- Careful scaling of all teeth should be performed with as little disruption of the tissue as possible. When significant periodontal pocketing is present, multiple appointments with gentle scaling and debridement are preferable to conventional deep scaling and root planing. When quadrant or multiple scaling sessions are necessary, the practitioner should allow a two-week period between appointments for tissue healing and gingival shrinkage to facilitate plaque and calculus removal.
- Ultrasonic scalers should not be used for extensive subgingival debridement to minimize irritation to the tissue. Hand scaling is preferred until ultrasonics can be used.
- Air polishers may be too disruptive to the soft tissues if misdirected, and should not be used, or if used, caution is advised.
- Polishing paste that is gritty or coarse should not be used because of irritation to the tissue both above and below the gingival margin.
- Tissue areas that do not respond to treatment may need further evaluation and possibly future biopsy.
- Mouth rinses containing alcohol should be avoided to prevent patient discomfort and tissue irritation. Some flavoring agents found in many dental products such as mint or cinnamon may act as an irritant to the tissues and should discontinued.
- Tarter control toothpaste and those with flavoring agents should be changed to a product such as XEROSTOM. Toothpaste free of additives such as sodium lauryl sulfate is recommended. Additionally, a children’s toothpaste is usually tolerated well with patients since these pastes have limited ingredients and tend to have less flavoring agents. These products are also highly effective in patients with xerostomia.
- Any polishing of the teeth should be performed using a mild paste such as the toothpaste currently used by the patient and this can be applied with a prophy cup. Gently brushing the teeth with the paste in the dental office will be of some benefit.
- We recommend the use of a soft bristle surgical brush such as the UltraSuave Red Brush or CURAPROX made with supersoft nylon bristles in cases where the mouth is too inflamed for routine oral hygiene. An appropriate surgical brush may be used. These can be used until the lesions are controlled and one is able to comfortably return to routine home care procedures.
- Patients should be instructed to discontinue the use of chewing gum, candy, mints, toothpastes, or mouth rinses that contain flavoring agents such as wintergreen, peppermint, spearmint, and cinnamon (cinnamon aldehyde).
- Floss is recommended and some patients prefer the interdental brushes that clean the proximal spaces between teeth very well. A water irrigation device is preferred by some clinicians and patients. These work well in dislodging food particles and disrupting the oral biofilm, but used on a low setting.
- Periodic oral digital photographs both for initial and for follow-up appointments are suggested. This allows better evaluation of treatment progress or lack of progress. Encourage patients to take photos with their cell phones or with their own digital camera so that the clinician has a good understanding of how the tissue responds between appointments.
- Encourage patients to document any tissue irritations and to keep a log of possible “trigger” mechanisms that may have caused lesions or irritations. The causes may be certain foods, beverages, changes in toothbrushes or oral care products, oral injury, stress etc.
Prepared by Dr. Terry Rees and Dr. Nancy W. Burkhart. January 27, 2021. Adapted from International Oral Lichen Support Group Web site, https://dentistry.tamhsc.edu/olp/
Tips for patients: Reducing stain on teeth
- Use a straw when drinking juices or liquids that stain the teeth.
- Add milk to tea/coffee to lessen the stain of the product.
- Rinse with clear water after eating or drinking a highly-pigmented food or drink such as coffee, tea, red wine or blueberries.
- Eat raw, crunchy type vegetables throughout the day.
- Some teas may stain more than others, changing to a less staining type such as white tea can decrease the stain.
- Hard cheeses may add a protective element to the teeth in fighting stains.
- Drinking hot water with lemon or flavors added to hot water such as fennel seeds, coriander, ginger and cumin (placed in a tea ball) can provide some of the same calming sensations as tea.
- The patient who drinks tea throughout the day might consider drinking tea followed by warm water with lemon for the next cup or perhaps a light herbal tea.
- Chewing gum with xylitol may diminish the stain by stimulating saliva to cleanse the mouth.
- Using a tongue cleaner to remove the residue on the tongue and in the papillae. The stain is continually bathing the teeth when left in the tongue papillae. Using a tongue cleaner several times a day is optimal.
- Specific instruction in brushing and flossing for the individual patient is necessary and may include an electric toothbrush as well as a manual brush along with an appropriate type of toothpaste. One that is recommended for the individual patient by a dental professional.
- Toothbrushes do not clean in between the teeth, so daily use of floss is optimal or interdental Proxabrush/or Soft-Picks.
- Depending upon the condition of the oral tissue, one of the new air flossers may even work for some individuals. Discuss their use with your dental hygienist/dentist.
Burkhart NW. Reduction of tooth stains: Patient education is vital to preventing tooth stain. RDH April 2015 5: (4) http://www.rdhmag.com/articles/print/volume-35/issue-4/columns/reduction-of-tooth-stains.html
July 2017
A message from Dr. Jairo Robledo-Sierra | DDS, MSc (OralMed), PhD
Thank you for the invite. In Sweden, where I was trained, they use clobetasol gel as a first-line corticosteroid treatment for OLP and other immune-mediated oral mucosal diseases, but I know that in the US, betamethasone is more commonly used. Clobetasol gel or mouthwash is not commercially available and is thus prepared by pharmacists with a prescription.
A few years ago, I wrote a fact sheet on OLP for a Swedish dental website (in Swedish). Here’s the part about treatment, which reflects the scheme that they use in Sweden, and I continue using in my Colombian patients:
In case of symptoms, the patient (with oral lichen planus) can be treated with clobetasol gel or mouthwash (0,025%), a potent corticosteroid, for six weeks.
Administration scheme:
- Weeks 1–2. Rinse with 10 ml of the gel/mouthwash for 2 minutes twice a day, together with nystatin to prevent the overgrowth of Candida. After the first two weeks, there is no need to continue using nystatin in most patients.
- Weeks 3–4. Rinse once in the evening using the same dosage.
- Weeks 5–6. Rinse every other evening using the same dosage.
If the patient has symptomatic gingival oral lichen planus (OLP), it is imperative to optimize oral hygiene before starting any pharmacological treatment.
If necessary, treatment can be continued with this dosage for about two months before the corticosteroid is withdrawn. The aim is to use as little clobetasol as possible to achieve symptom relief. However, patients with severe OLP may be allowed to take the medication once a day for several months before reducing the dosage.
Jairo Robledo-Sierra | DDS, MSc (OralMed), PhD
Associate Professor | Faculty of Dentistry
CES University | Calle 10A # 22 - 04 | Medellín, Colombia
Tel: (57) (4) 444 05 55 Ext. 1603 | Fax: (57) (4) 311 35 05